by Kelly Kordom
Traumatic brain injury (TBI) refers to injury to the brain via an external force and is one of the leading causes of mortality and morbidity in children worldwide. Given that children are a vulnerable group to research it initially seemed appropriate to extrapolate clinical findings from research including adult populations to the paediatric cohort. Ironically though this review paper by Professor Anthony Figaji highlights how the lack of data available for the treatment of paediatric TBI makes it increasingly difficult to appropriately treat this vulnerable population. The paper indicates that the anatomical and physiological differences between children and adults also manifest in the injuries sustained as a result of TBI and the clinical interventions that need to take place.
Anatomically the head of a children is relatively large compared to the size of their body and given that their neck muscles are also weaker they are more vulnerable to severe injury during TBI, particularly at the craniospinal region. It has been demonstrated that younger children are more likely to experience spinal cord injury without radiographic abnormality and diffuse injuries are also more common within the paediatric cohort. This is of particular concern, because it is therefore more difficult to identify these injuries in common imaging techniques such as CT scans or MRIs.
It is also important to note that during the first 18 months of life one’s skull is still malleable and undergoes a lot of change. It has been demonstrated that this does allow for some buffering in monitoring intracranial pressure (ICP), however its compliance can be short lived and bring about adverse effects. Compliance also depends on the ratio of cerebrospinal fluid to brain volume and cerebral blood flow, and additionally the research suggests that this is all age dependent. This further highlights that post severe TBI, we cannot rely on ICP thresholds based on adult populations, especially considering that currently there is still controversy on ICP thresholds for adults.
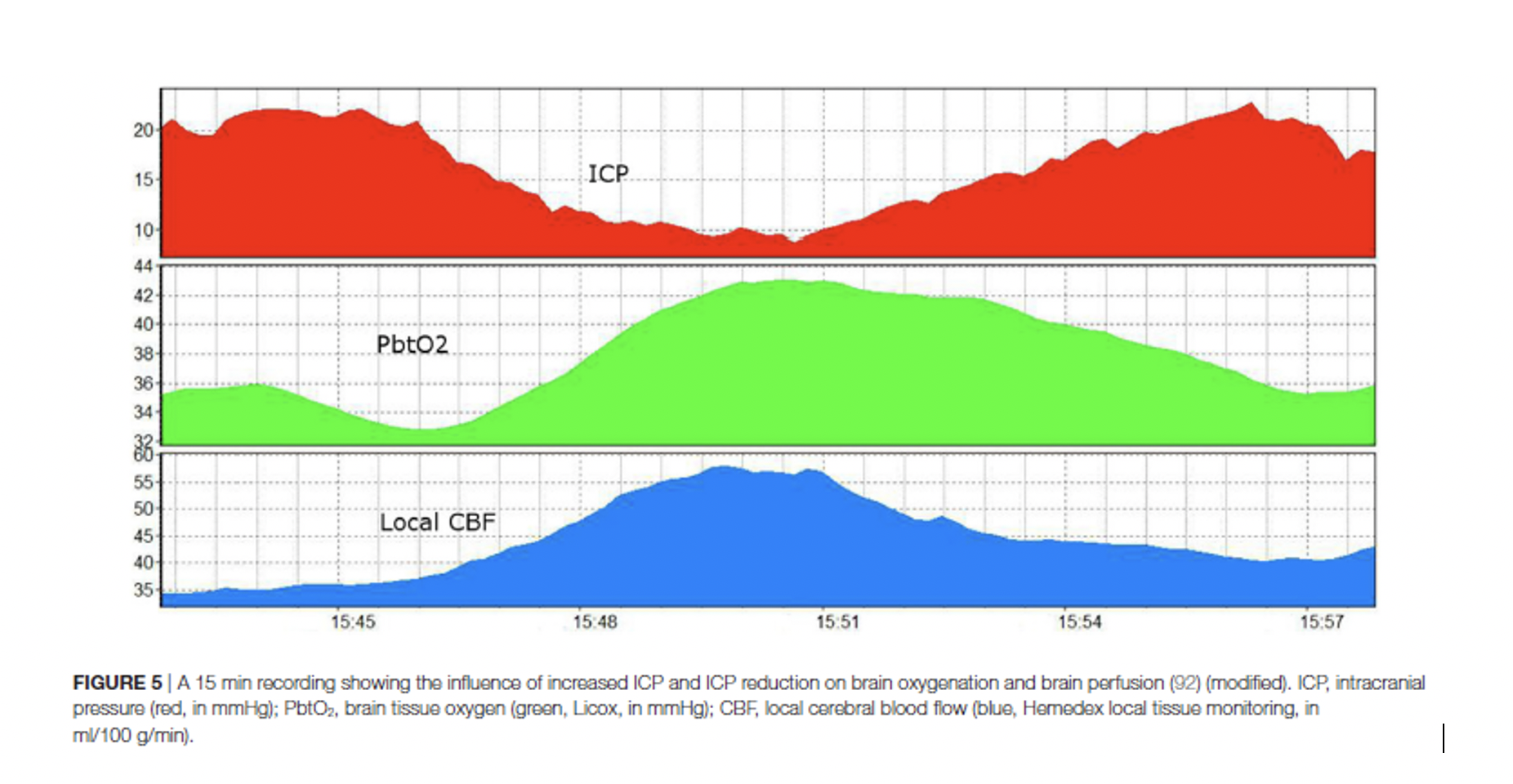
As it is now there is limited evidence and research on therapies and treatment interventions that are specific for paediatric TBI, however ICP monitoring has provided researchers and clinicians with more information on how to interpret the data and how to respond. Figure 5 (below) from the article as shown below is an example of what ICP monitoring looks like and indicates how an increase or decrease in ICP affects other parameters such as brain oxygenation and local cerebral blood flow.
Even though it has been reported that children generally have better developmental outcomes it is worth recognizing that some injuries sustained during TBI are long lasting as their brains are still developing and the ongoing activation of inflammatory processes may only manifest as clinical symptoms later in life. At this point the research on paediatric TBI or lack thereof is currently preventing clinicians from providing perhaps more efficient and appropriate care to children who are affected.
Reference
Figaji, A., 2017. Anatomical and Physiological Differences between Children and Adults Relevant to Traumatic Brain Injury and the Implications for Clinical Assessment and Care. Frontiers in Neurology, 8, pp1-15.

Leave a comment