by Mandisa Mabaso
Introduction
The Pulmonary veins transport oxygenated blood from the lungs to the left atrium of the heart. They are mainly located in the interlobular septa and drain each bronchopulmonary segment on the anterior surface of the bronchus. In addition, veins run between the segments, mediastinal, and fissural surfaces. Often, the veins of the middle lobe of the inferior lobe arise from those of the right medial. In addition, the right superior and middle pulmonary veins drain the right superior and middle lobes, while the right inferior and left inferior pulmonary veins drain the corresponding inferior lobes.
Aim
The aim of the study is to determine the incidence of different draining patterns of the right pulmonary vein at the hilum.
Methods
The study involved twenty-six formalin-fixed adult cadaveric lungs from Bangalore Medical College & Research Institute. The dissection initially involved identifying the structures at the hilum. Additionally, the pulmonary veins were picked up and their tributaries were traced peripherally by carefully dissecting the lung tissue using blunt forceps. Therefore, different patterns in the drainage of the pulmonary veins were noted.
Results
In 53.8% of dissected lungs, the right superior lobar vein and middle lobar vein unite to form the right superior pulmonary veins, Moreover, the right superior lobar vein drained the apical and anterior segments of the right upper lobe and also the medial and lateral segment of the right middle lobe from the anterior surface, whereas veins from the posterior segment of the upper lobe drained into the posterior aspect of the superior pulmonary vein. These lungs fall under Type A, whereby the right superior lobar vein (RSLV) and right middle lobar vein (RMLV) join to form the right superior pulmonary vein (RSPV) as seen in Figure 1.

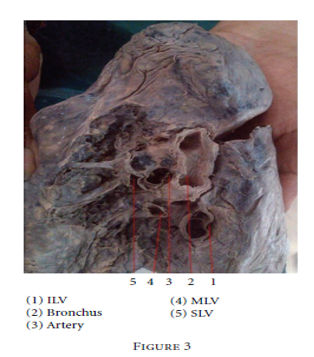
In 26.6% of dissected lungs, the right superior lobar vein and the right middle lobar vein did not join, and all three lobar veins drained separately at the hilum. This belongs to Type B, whereby the right superior lobar vein (RSLV), right middle lobar vein (RMLV), and right inferior lobar vein (RILV) drain separately in Figure 3.
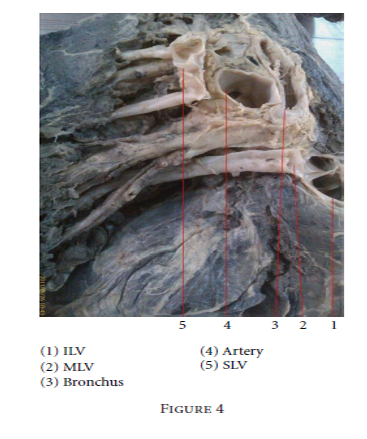
In 11.53% of dissected lungs, the right superior lobar vein received tributaries from the right upper lobe, whereas the right middle lobar vein joined with the inferior lobar vein to form the right inferior pulmonary vein (Figure 4). This belongs to Type C, where RSLV forms RSPV, and RMLV and RILV join to form the right inferior pulmonary vein (RIPV).
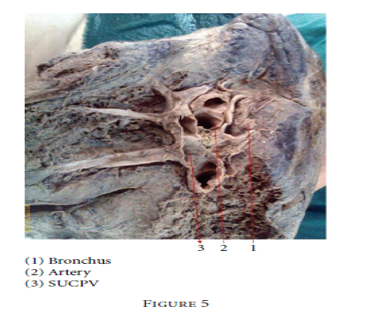
In 3.8% of dissected lungs, the right superior lobar vein, the right middle lobar vein, and the right inferior lobar vein drained into a common vein forming the right single unilateral central pulmonary vein (Figure 5). This belongs to Type D, where RSLV, RMLV, and RILV join to form the right unilateral single central pulmonary vein (RUSCPV).
Discussion
This study focuses on the drainage patterns of the right lung’s pulmonary veins, focusing on all three lobar veins which are RSLV, RMLV, and RILV. Variations in the vein numbers and course are common, and patients with separate ostium for the right middle lobar vein have higher atrial arrhythmia frequency as seen in Figure 3. Anomalysed veins can lead to the right ventricular diastolic overload, causing ectopic beats. Understanding the normal pulmonary venous anatomy is essential for pre-ablation planning and for the evaluation of post-ablation complications. Pulmonary veins trigger atrial fibrillation in patients with paroxysmal atrial fibrillation, and catheter ablation is a treatment strategy targeting these triggers. In addition, anatomic variation of the middle lobar vein draining into the inferior pulmonary vein is important for the right lobar lobectomy surgery.
Conclusion
The study found significant variations in pulmonary venous anatomy in 46.03% of dissected lungs, aiding in the classification of anatomical patterns based on drainage patterns of the right pulmonary vein at the hilum. The results confirm that there is considerable variation in the anatomy of pulmonary veins. Moreover, with the increasing use of cardiovascular imaging, variations in the pulmonary vein anatomy have become more appreciated, hence detailed knowledge of pulmonary venous anatomy and drainage patterns is important during mapping and ablation procedures.
References
Rajeshwari, M. S., & Ranganath, P. (2012). Variations in draining patterns of right pulmonary veins at the hilum and an anatomical classification. International Scholarly Research Notices, 2012.


Leave a comment